Chapter I
My “Journey to Cure”
Excerpt from Journey to Cure
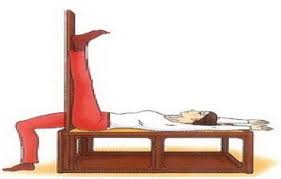
Like yesterday, I put out low tables at the corridor outside for the queuing Tibetans to do Lajin. The number of tables had increased from three to six, on top of each lay a patient, who had one leg straight up against the pole, while someone next to him helped to press his legs. If I noticed that some did not seem to benefit from the practice, I would make them repeat it, with me pressing the leg, and showing those around how painful the facial expression would be when it was done properly. In the end, they realized that their symptoms had gone with the painful exercise.

Helping to press legs of the one doing Lajin
n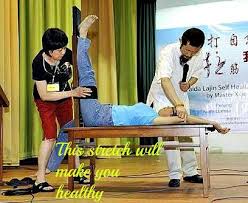
My “Journey to Cure”
Excerpt from Journey to Cure
Like yesterday, I put out low tables at the corridor outside for the queuing Tibetans to do Lajin. The number of tables had increased from three to six, on top of each lay a patient, who had one leg straight up against the pole, while someone next to him helped to press his legs. If I noticed that some did not seem to benefit from the practice, I would make them repeat it, with me pressing the leg, and showing those around how painful the facial expression would be when it was done properly. In the end, they realized that their symptoms had gone with the painful exercise.
Helping to press legs of the one doing Lajin
n
It really made my day when I witnessed the immediate effects of Lajin — it not only cured the pain
in the torso and limbs, but also eased headaches and pains in internal organs. A woman who had
pain in her knees and legs had it eliminated after Lajin, but the pain in her back, chest and
stomach remained. There were clicking sounds in her thoracic and lumbar vertebrae when I
performed bone-setting on her, after that all her remaining pain disappeared; in another case, I
used bone-setting on a middle-aged man with acute stomach pain that radiated from his abdomen
to the back. After four popping sounds on his thoracic vertebrae, the pain went away completely.
By now I was convinced that pain in the organs such as stomach and liver must be closely related
to the corresponding spots on the vertebrae.
It occurred to me that since Lajin could easily be practiced at home or in the office, it should be introduced to the world so that more people could benefit from it, especially the increasing number of office workers who suffer from neck and back pains. Companies could consider installing “Lajin benches” in the office, as part of employee benefits package.
I also discovered some sad truths today. I saw that some Tibetans had spent the night sleeping along the corridor of the monastery, in order to get treated the next day. From this I guessed that the reason why so many Tibetans suffer from diseases such as arthritis might be because a majority of them are nomads used to sleeping out in the fields at night where damp and cold air gets into the body. Since there are hardly any medical services available at remote places in Tibet, people could not get treated when sick; instead, they have to rely on such drugs as painkillers or hormone pills, which they could buy without prescription. Monasteries with many lamas usually purchase boxes of painkillers so as to alleviate various pains. The overdose and/or misuse of these medicines induce a lot of diseases, such as distortion of bones. Deafness, which is a common illness here, is caused by misuse of hormone drugs to treat colds. To make things worse, a lot of drugs sold to the locals here are either counterfeit or of poor quality, which nobody elsewhere would take.
Many illnesses can actually get treated without any medication, including the many eye problems I found among my patients, such as cataract, far-sightedness, inflamed or tearing eyes, because they could all be cured with acupuncture. However, due to poverty and lack of acupuncturists in the area, people either let it worsen, or travel afar to a hospital to get infusions. They seemed to be always getting infusions in hospital, and hardly receiving any other treatments. Sadly, they seemed to always get sicker after the infusions.
Excerpt from Journey to Qinghai
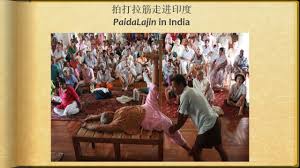
Paida and Lajin in the Sun
After lunch, we went back to the kitchen. Again, it was overcrowded. I had to invite those waiting their turns out. I laid out a few more tables and encouraged them to do Lajin. The first two men about to receive treatment both had lower back pain and hip pain, and were limping. I asked, “Have you done Lajin?” They both answered, “Yes.” “Have you done Paida?” I asked. “Yes.” “Have you patted your hip?” I asked again. “No.” was their answer. As they were men (hence would not be embarrassed to expose the hip), I asked them to take off their pants to have the hip patted.
One of them, while loosening his pants, pointed to his ass and asked, “It was patted yesterday. Doesn’t that count?” I took a look — there was a large area of purple Sha (poisoned blood). I asked, “Is your pain relieved?” “Yes.” He answered. I took the opportunity to explain to him, “The purplish dark Sha shows that Paida is effective on you, and the cold-dampness (chills in the body that induce various diseases) is being cleared. You need to continue receive heavy Paida.” I asked another man to pat his hip. But his Paida was way too gentle. I showed him how to pat vigorously. Everyone laughed. The one helping to Paida took the hint and began to use heavy slaps. The one receiving Paida immediately showed painful expressions.
The other sturdy Kangba man had to follow suit, and took off his pants to receive Paida. Very soon a large area of Sha appeared on his hip. I said to them, “It’s best to pat yourself, as you’ll be both the giver and receiver of this ‘gift’.” In the beginning, they were reluctant to pat themselves. I explained to them why and they began to use genuine slaps. Over time, they got slack, with arms rising and falling slowly and the intensity falling, just like the lazy kowtow machine in an oilfield. From time to time, I had to ask others to give them a few hard slaps. It went on like this for half an
It occurred to me that since Lajin could easily be practiced at home or in the office, it should be introduced to the world so that more people could benefit from it, especially the increasing number of office workers who suffer from neck and back pains. Companies could consider installing “Lajin benches” in the office, as part of employee benefits package.
I also discovered some sad truths today. I saw that some Tibetans had spent the night sleeping along the corridor of the monastery, in order to get treated the next day. From this I guessed that the reason why so many Tibetans suffer from diseases such as arthritis might be because a majority of them are nomads used to sleeping out in the fields at night where damp and cold air gets into the body. Since there are hardly any medical services available at remote places in Tibet, people could not get treated when sick; instead, they have to rely on such drugs as painkillers or hormone pills, which they could buy without prescription. Monasteries with many lamas usually purchase boxes of painkillers so as to alleviate various pains. The overdose and/or misuse of these medicines induce a lot of diseases, such as distortion of bones. Deafness, which is a common illness here, is caused by misuse of hormone drugs to treat colds. To make things worse, a lot of drugs sold to the locals here are either counterfeit or of poor quality, which nobody elsewhere would take.
Many illnesses can actually get treated without any medication, including the many eye problems I found among my patients, such as cataract, far-sightedness, inflamed or tearing eyes, because they could all be cured with acupuncture. However, due to poverty and lack of acupuncturists in the area, people either let it worsen, or travel afar to a hospital to get infusions. They seemed to be always getting infusions in hospital, and hardly receiving any other treatments. Sadly, they seemed to always get sicker after the infusions.
Excerpt from Journey to Qinghai
Paida and Lajin in the Sun
After lunch, we went back to the kitchen. Again, it was overcrowded. I had to invite those waiting their turns out. I laid out a few more tables and encouraged them to do Lajin. The first two men about to receive treatment both had lower back pain and hip pain, and were limping. I asked, “Have you done Lajin?” They both answered, “Yes.” “Have you done Paida?” I asked. “Yes.” “Have you patted your hip?” I asked again. “No.” was their answer. As they were men (hence would not be embarrassed to expose the hip), I asked them to take off their pants to have the hip patted.
One of them, while loosening his pants, pointed to his ass and asked, “It was patted yesterday. Doesn’t that count?” I took a look — there was a large area of purple Sha (poisoned blood). I asked, “Is your pain relieved?” “Yes.” He answered. I took the opportunity to explain to him, “The purplish dark Sha shows that Paida is effective on you, and the cold-dampness (chills in the body that induce various diseases) is being cleared. You need to continue receive heavy Paida.” I asked another man to pat his hip. But his Paida was way too gentle. I showed him how to pat vigorously. Everyone laughed. The one helping to Paida took the hint and began to use heavy slaps. The one receiving Paida immediately showed painful expressions.
The other sturdy Kangba man had to follow suit, and took off his pants to receive Paida. Very soon a large area of Sha appeared on his hip. I said to them, “It’s best to pat yourself, as you’ll be both the giver and receiver of this ‘gift’.” In the beginning, they were reluctant to pat themselves. I explained to them why and they began to use genuine slaps. Over time, they got slack, with arms rising and falling slowly and the intensity falling, just like the lazy kowtow machine in an oilfield. From time to time, I had to ask others to give them a few hard slaps. It went on like this for half an
hour, and indeed their hip pain was greatly eased. I asked them to walk again, and they could
basically do it normally. They couldn’t help but feel amazed at the healing method and its
wonderful efficacy.


Helping each other do Lajin
Taken from Mr. Xiao’s blog:
h t tp : / / b lo g . s i n a . c o m . c n / s / b lo g _ 5 dc 9 4 6 a 6 0 1 0 0 h 3 e 5 . h tm l
English version posted at E-Tao website:
h t tp : / / w w w . P a i da L a j i n . c o m / e n / h o m e / m _ p o s t . a s p ? i d = 2 1 3 7 9 5 5 1 8 1 4 9
Editor’s Note:
Taken from Mr. Xiao’s blog:
h t tp : / / b lo g . s i n a . c o m . c n / s / b lo g _ 5 dc 9 4 6 a 6 0 1 0 0 h 3 e 5 . h tm l
English version posted at E-Tao website:
h t tp : / / w w w . P a i da L a j i n . c o m / e n / h o m e / m _ p o s t . a s p ? i d = 2 1 3 7 9 5 5 1 8 1 4 9
Editor’s Note:
Paida in a group
Visit our website at http://www.paidalajin.com/en/home/ to read more of Mr. Hongchi Xiao’s
“Journey to Cure” stories. You can also get free downloads, watch videos, read FAQs and self-healing
stories from around the world.
